




Findings
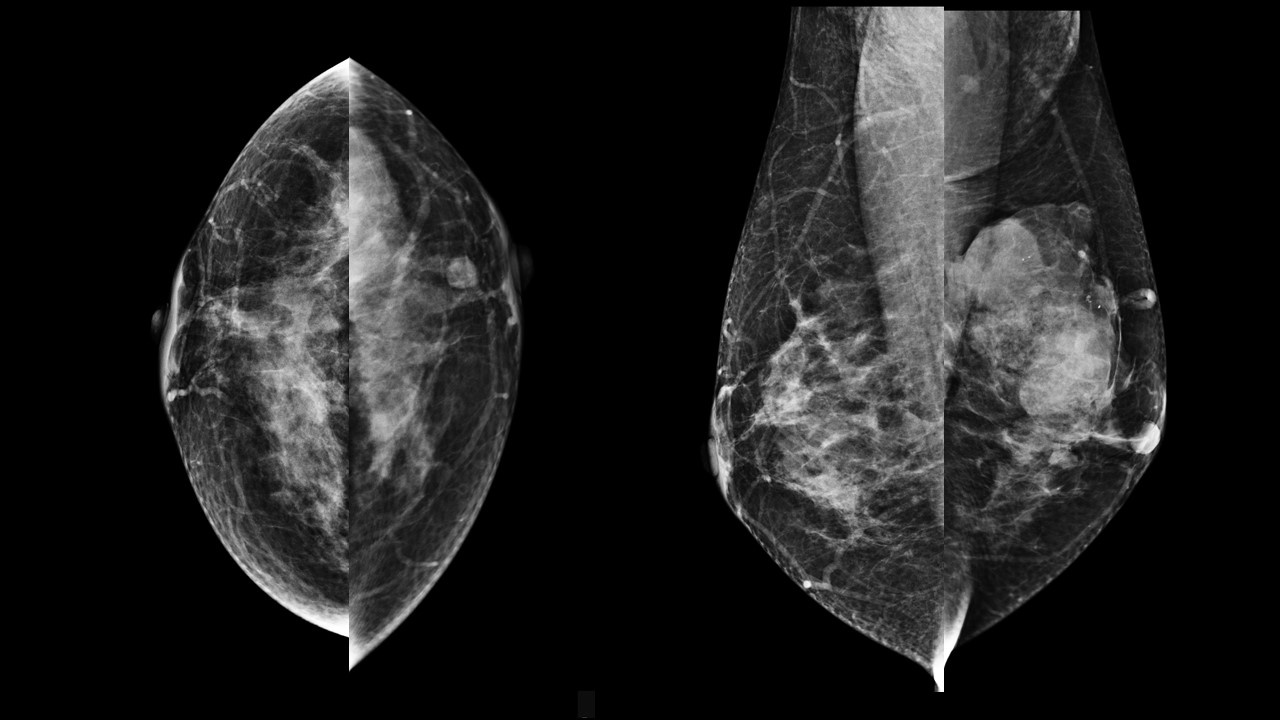
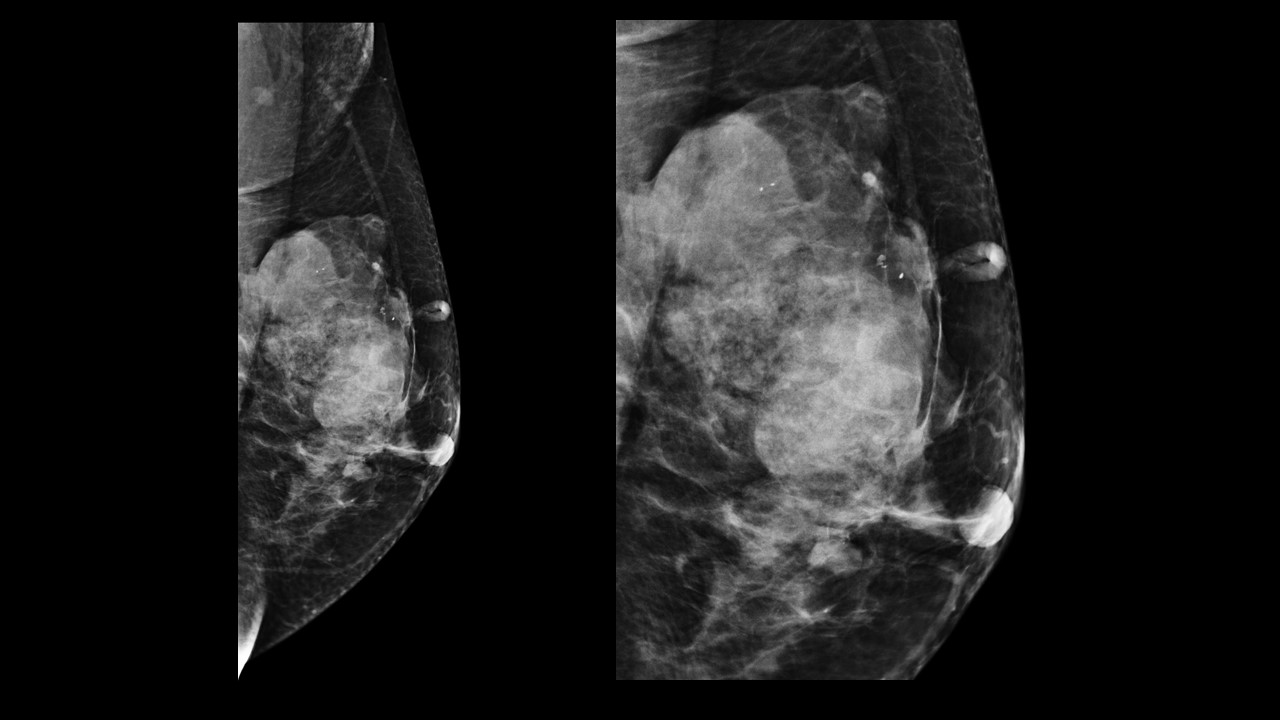
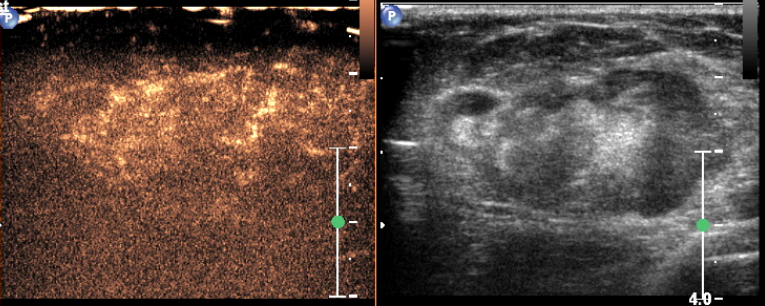
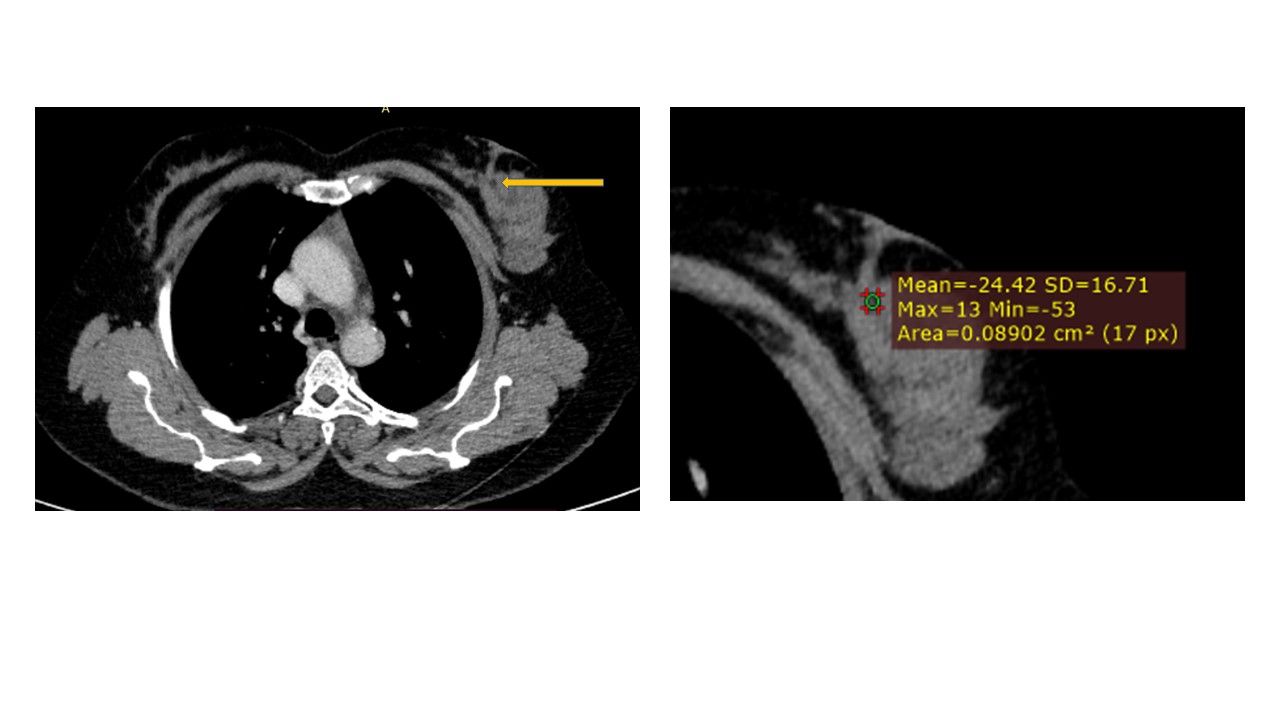
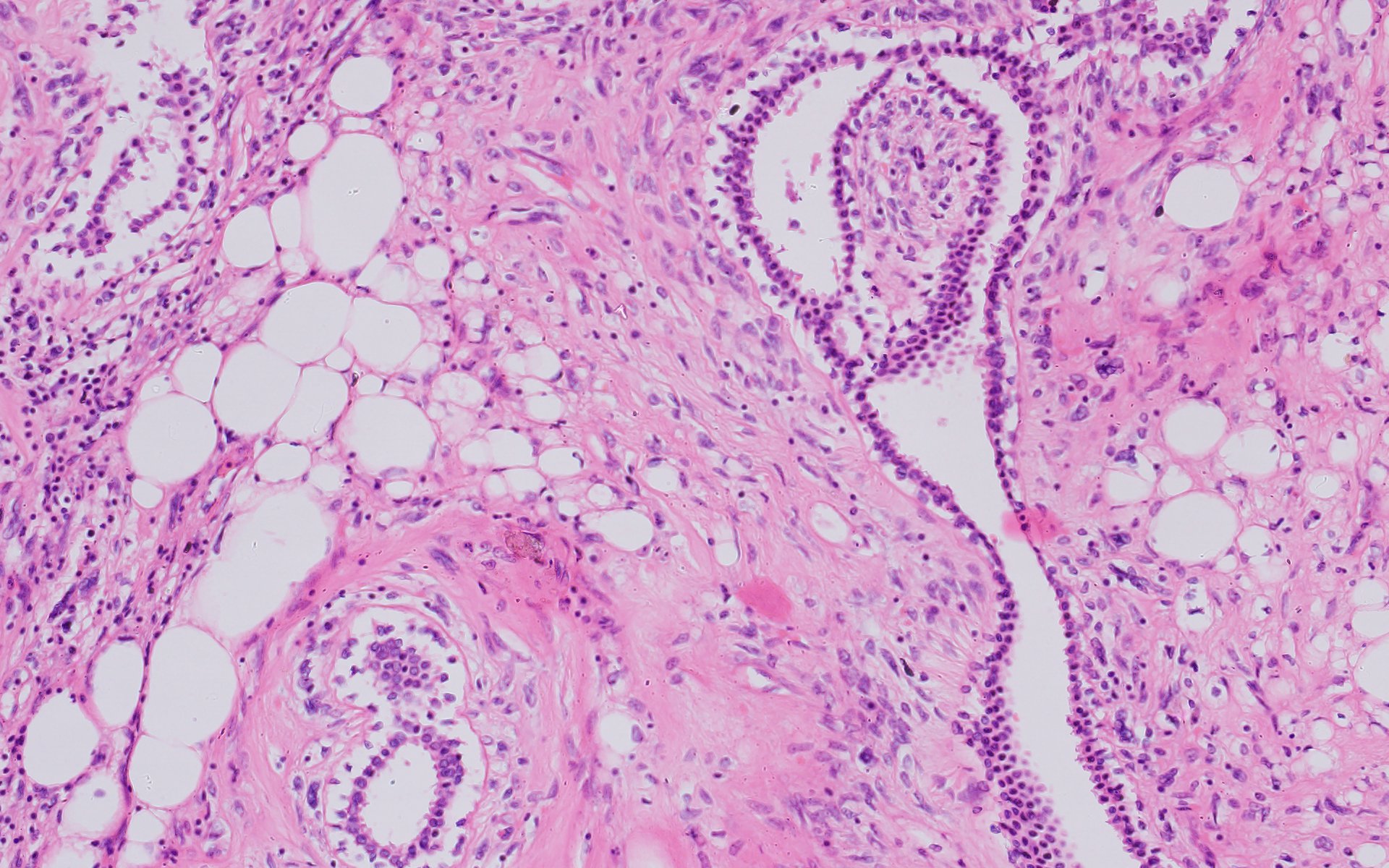
Mammography demonstrated an irregular, fat-containing, heterogeneous mass with circumscribed margins in the upper outer quadrant of left breast. Few scattered foci of coarse calcification were present within the mass. Breast sonography revealed an irregular, parallel, hyperechoic mass with circumscribed margins and no posterior acoustic features in the left breast at 3 o’clock position. Mild vascularity was observed on Color Doppler imaging. Contrast enhanced ultrasound (CEUS) done out of academic interest showed ill-defined, heterogenous enhancing mass, showing irregular shape, having surrounding vessels. Quantitative analysis showed higher PI (pulsatility index), AUC (area under curve) and lower TTP (time to peak) compared to normal tissue. The mass was assessed as Breast Imaging Reporting and Data System category 4b, and ultrasound-guided 14-gauge core biopsy revealed a biphasic tumor composed of bilayered ductal epithelium compressed by the proliferating stroma into leaf like architecture, The stromal cells showed increased cellularity, marked nuclear atypia and pleomorphism with round to oval nuclei, opened up chromatin, prominent nucleoli and moderate to abundant cytoplasm with many bizarre looking tumor giant cells. The stroma showed extensive heterologous lipomatous differentiation composed of neoplastic adipocytes as well as few lipoblasts. Mitosis was 3-4/10/hpf. Final histopathological diagnosis of malignant Phyllodes tumor with liposarcomatous differentiation was given. CT scan chest was done to look for lung metastasis, which revealed an irregular soft tissue mass in left breast with internal focal areas of fat attenuation. No nodules were seen in the lungs. Subsequent lumpectomy was performed and the gross specimen showed a well-demarcated tumor, measuring 6.8 × 6.5 × 3 cm. There were considerable bright yellow fatty components and some cleft-like spaces. Microscopically, the tumor exhibited a typical leaf-like growth pattern with extensive stromal overgrowth and stromal hypercellularity. Extensive areas of lipomatous differentiation were seen ranging from mature adipocytes to lipoblasts showing marked stromal atypia and irregularity. Mitotc activity was 7-8/10hpf. IHC for MDM2 was negative. Overall features were of malignant phyllodes tumor with well differentiated liposarcomatous differentiation.
Answer
Malignant phyllodes tumor with well differentiated liposarcomatous differentiation.
Discussion
Phyllodes tumors account for less than 0.3-1% of all breast neoplasms. They are rare fibroepithelial neoplasms of the breast, more commonly seen in middle-aged women. The most common presentation is that of a rapidly growing, palpable mass. Phyllodes tumors may be classified as benign, malignant, or borderline, a distinction which is largely made histologically based on the degree of nuclear atypia, tumor border, stromal cellularity, and mitotic activity. While Ductal carcinoma in situ (DCIS), Lobular carcinoma in situ (LCIS), or invasive cancers may arise from the epithelial component of phyllodes tumors, the stromal component may contain heterologous elements such as adipose tissue, cartilage, bone, skeletal muscle, and fibrous tissue. Lipomatous differentiation within a phyllodes tumor is an uncommon stromal alteration. Malignant phyllodes tumor usually differentiates into fibrosarcoma, with liposarcomatous differentiation rarely being reported. IMAGING: On mammography, phyllodes is typically seen as non-specific large rounded oval or lobulated, generally well circumscribed mass with smooth margins. A radiolucent halo may be present. Calcification (typically coarse and plaque like) may be seen in a very small proportion. General sonographic features are non-specific and can mimic that of a fibroadenoma. On ultrasonography (USG), most of these tumors are hypoechoic, have circumscribed margins and may exhibit posterior acoustic enhancement. A solid mass containing round or cleft like cystic spaces and demonstrating posterior acoustic enhancement strongly suggests the diagnosis of phyllodes tumor. Vascularization is usually present in the solid components. On MRI, signal characteristics can vary with histological grade, but in general most of these are usually of low signal on T1, can be variable ranging from homogenous low to high signal on T2 and the solid components enhance after contrast administration on T1 C+ (Gd). DIFFERENTIAL DIAGNOSIS: Given the extensive fat present within the mass on imaging, differential diagnosis of the current case includes hamartoma, which is a benign, well-circumscribed tumor composed of all components of breast tissue (fibrous, fibrocystic, and adipose tissue), resulting in a “breast-within-a-breast" appearance on mammography. Histologically, disordered breast ducts and lobules are present, unlike the phyllodes tumor which has epithelium lined spaces and stromal overgrowth. Another differential diagnosis is a primary liposarcoma which should only be diagnosed after thorough sampling has excluded a phyllodes tumor. Additional differential considerations include metaplastic carcinoma, primary breast sarcoma, and periductal stromal sarcoma which are largely distinguished histologically. Treatment of malignant phyllodes tumors of the breast requires complete surgical excision with tumor-free margins. The impact of adjuvant chemotherapy and radiotherapy has been reported to be variable. TEACHING POINTS • Hyperechoic breast masses have a high predictive value for benignity; however several malignant lesions of the breast like lymphoma, angiosarcoma, and metastases may present as hyperechoic masses. • Though there is substantial overlap in the sonographic and mammographic features of benign, borderline, or malignant phyllodes tumors; predictors of increased risk of borderline or malignant phyllodes tumors are patient’s age (>55 years), irregular lesion shape, partially obscured or indistinct tumor margins and size >3 cm. • Knowledge of sonographic and mammographic findings of this rare breast neoplasm can help to avoid late diagnosis and serve as a reminder that hyperechoic breast lesions are not always benign.
Reference
1. Ji Hee Kim and Ji Young Lee: Malignant phyllodes tumor of the breast with liposarcomatous differentiation: A case report with imaging findings. Radiol Case Rep. 2019 May; 14(5): 531–34