

Findings
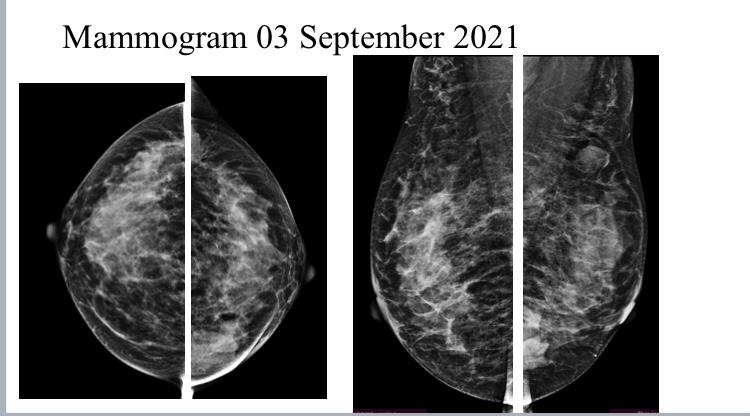
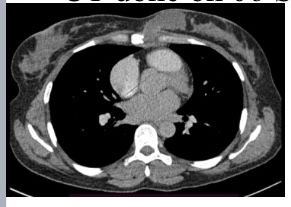
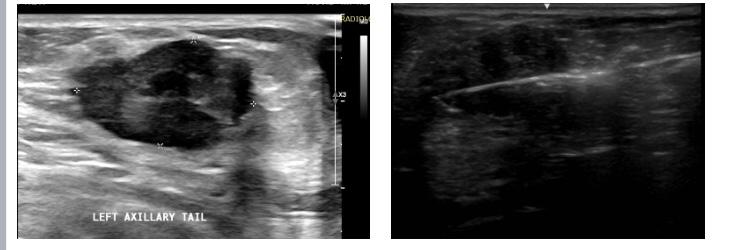
Mammogram Left MLO view shows a circumscribed high-density round to oval lesion in the upper quadrant near the axillary tail. Another partially visible high-density lesion is seen in the lower inner quadrant posterior third of the breast ( retroglandular zone) near the chest wall. Corroborative USG of the upper outer quadrant lesion revealed a hypoechoic round to oval lesion with microlobulated margins while the lower inner quadrant lesion revealed an anechoic collection with fine internal echoes reaching up to the chest wall with areas of bone erosion of the sternum. CT was done to see the extent of collection and other lesions which showed a hypodense collection in the chest wall near the sternum with areas of bone erosion and a hypodense round to oval lesion near the axillary tail. PET CT was done for academic purposes which showed uptake from the chest wall lesion near the sternum with no uptake in the hypodense collection. Biopsy was done from both the upper outer quadrant and chest wall lesion.
Answer
Left upper outer quadrant lesion— fibroadenoma Lower inner quadrant chest wall TB with intramammary abscess.
Discussion
Tuberculosis of the Chest wall constitutes less than 5% of all cases of musculoskeletal tuberculosis (1-4). Musculoskeletal tuberculosis is far less frequent in comparison to pulmonary mycobacterial infections and constitutes around less than 2% of tuberculosis cases overall. (5-7). Breast tissue is relatively resistant to mycobacterial infections. (8) In the chest wall tuberculosis has a predilection for the sternum, rib shaft, costochondral junctions, and vertebrae(9). The duration of the presenting symptoms in breast TB is usually less than a year but may vary from a few months to several years. (10,11) In our patient, ultrasound was helpful in revealing the lower inner quadrant lesion as an abscess. CT showed the extent of the collection in the chest wall adjacent to the sternum and also the lytic areas in the sternum and ruled out other lesions. Tuberculosis diagnosis requires microbiological confirmation for which needle aspiration and biopsy of both lesions can be done. PET CT holds a supportive role in diagnosis mainly to rule out malignancy in atypical cases. In our case, mild uptake was seen in the sternum near the site of the abscess. Extrapulmonary TB occurring in the breast is rare and presentation as a painless breast lump, as in our case, is unusual. Our case highlights the importance of mammograms in detecting extramammary disease which may involve the breast secondarily. This case also illustrates how different modalities complement each other to narrow the diagnosis while histopathology remains the final answer to suspicion
Reference
1. Bannerjee SN, Ananthakrishran N, Mehta RB. Tuberculous mastitis: a continuing problem. World J Surg 1987; 11:105-9. 2. Hulnick DH, Naidich DP, McCauley DI. Pleural tuberculosis evaluated by computed tomography. Radiology 1983; 149:759-65. 3. Gayler BW, Donner MW. Radiographic changes of the ribs. Am J Med Sci 1967; 253:586-619. 4. Mathlouthi A, Ben M'Rad S, Merai S, et al. Tuberculosis of the thoracic wall. Presentation of 4 personal cases and review of the literature. Rev Pneumol Clin 1998; 54:182-6. 5. EidA, ChaudryN, el-GhorouryM, et al. Multifocal musculoskeletal cystic tuberculosis without systemic manifestations. Scand JInfect Dis 1994; 26:761-4. 6. Garcia S, Combalia A, Serra A, Segur JM, Ramon R. Unusual locations of osteoarticular tuberculosis. Arch Orthop Trauma Surg 1997; 116:321-3. 7. Chang DS, Rafii M, McGuinness G, Jagirdar JS. Primary multifocal tuberculous osteomyelitis with involvement of the ribs. Skeletal Radiol 1998; 27:641-5. 8. Alagaratnam TT, Ong GB. Tuberculosis of the breast. Br J Surg 1980;67:125-6. 9. Morris BS, Varma R, Garg A, Awasthi M, Maheshwari M. Multifocal musculoskeletal tuberculosis in children: appearances on computed tomography. Skeletal Radiol 2002; 31:1-8. 10. Dubey MM, Agrawal S. Tuberculosis of the breast. J Indian Med Assoc 1968; 51:358-9. 11. Mukerjee P, George M, Maheshwari HB, Rao CP. Tuberculosis of the breast. J Indian Med Assoc 1974; 62:410-2.