

Findings
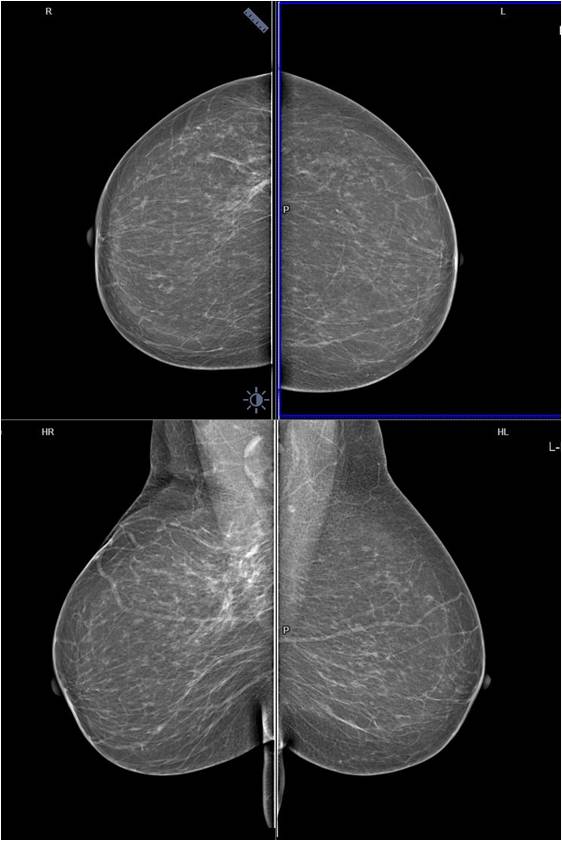
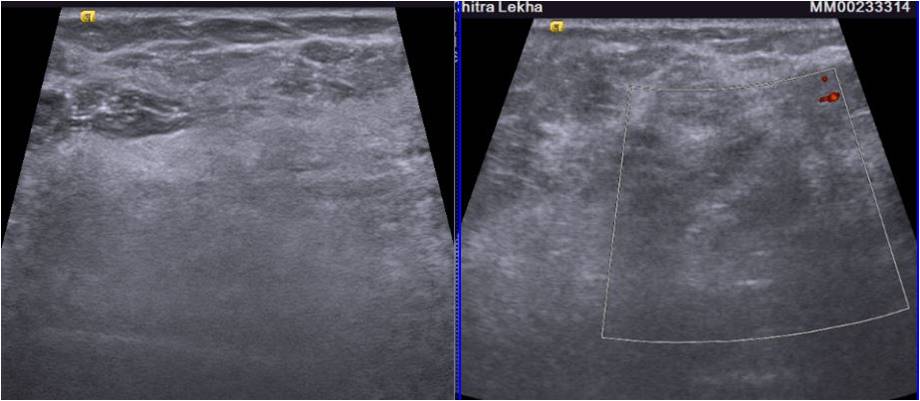
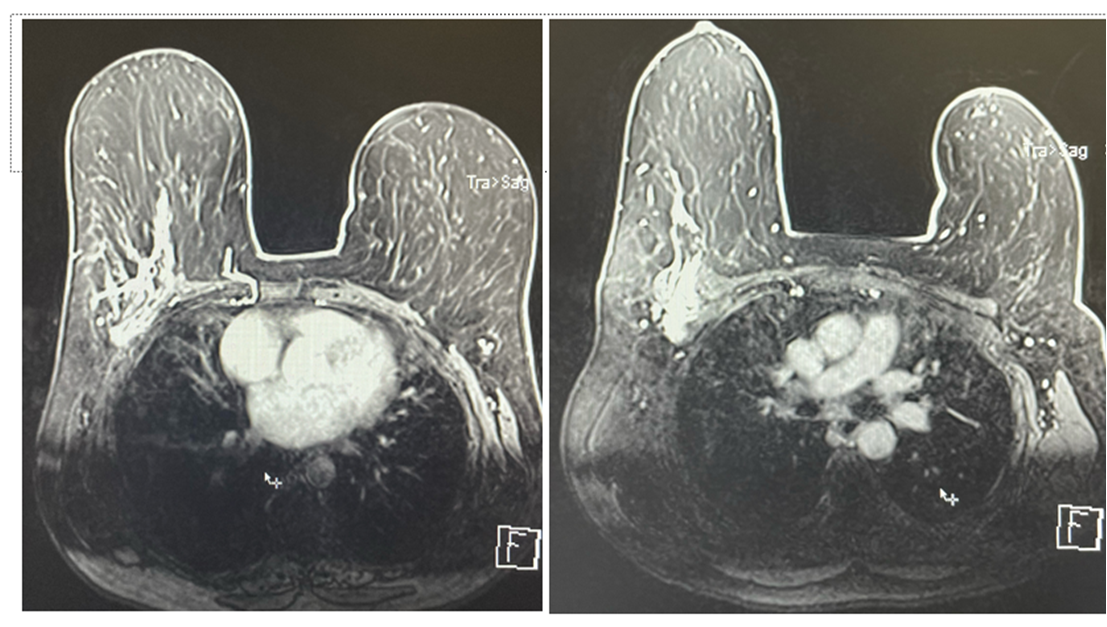
Screening mammogram MLO view revealed an area of focal asymmetry in the right breast in the form of multiple linear densities involving the upper outer quadrant. Spot compression CC view in the area of focal asymmetry shows that the asymmetric density does not disappear on compression. •A prominent axillary lymph node is seen with maintained fatty hilum and normal cortical thickness. A High-resolution Ultrasound of the breast showed an ill-defined area of hyperechogenicity in the right upper outer quadrant. No significant internal vascularity was seen on color doppler images. On contrast enhanced MR images a large area of heterogeneous, non mass like enhancement is seen in regional distribution involving upper outer quadrant of right breast. Linear extension of enhancement is seen in breast parenchyma with intervening normal breast tissue. Infiltration of underlying pectoral muscles is also noted. Ultrasound guided biopsy is done on the account of the presence of suspicious Imaging findings. The area of focal asymmetry on mammography revealed multiple linear shadows On ultrasound, an area of focal abnormal hyperechogenicity with indistinct margins was seen. The lesion was ill-defined with non circumscribed margins which raised the suspicion of a sinister pathology. Contrast enhanced MRI breast was performed to assess nature and extent of disease. It confirmed the infiltrative nature of the disease and involvement of the pectoralis muscle •On histopathology, a diagnosis of invasive lobular carcinoma was made. The node’s FNAC revealed a reactive node
Answer
Final diagnosis - Invasive lobular carcinoma. Differential diagnosis for echogenic malignant breast lesions include ductal carcinoma in situ, invasive lobular carcinoma, angiosarcoma, lymphoma, and metastasis to the breast.
Discussion
Invasive lobular carcinoma (ILC) is the second most common histologic type of breast carcinoma after IDC and is associated with a higher rates of multiplicity and bilaterality. •ILC are difficult to identify clinically and pose a diagnostic dilemma as well and are usually detected at a later stage, increasing the likelihood of large primary lesions and positive node status at biopsy. Even in our case the mass was neither palpable, nor had typical features of malignancy on screening mammography, in fact hyperechogenicity on the ultrasound was quite reassuring. So knowledge of possibility of vague appearances in case of ILC and low threshold for biopsy is needed to reach to the diagnoses •Although the most common mammographic presentation of ILC is a high density spiculated mass, ILC is often difficult to diagnose on the mammogram and may manifest as atypical findings including architectural distortion, masses with poorly defined margins, focal asymmetry, circumscribed masses, and even a negative mammogram. The masses and asymmetry associated with , have an opacity less than or equal to that of normal breast parenchyma and the tumor often lacks the central density. The nature of architectural distortion is often very subtle. These findings make it very difficult to detect on a mammogram •ILC is composed of non-cohesive tumor cells which characteristically spreads by diffuse infiltration of single rows of malignant cells in a manner that does not destroy underlying anatomic structure or elicit a substantial desmoplastic response. It may spread along the stroma of the breast like a spider’s web. So although it involves a large area but still may not be felt or well seen on conventional imaging •Micro-calcifications are far less common in the ILC as compared to invasive ductal carcinomas. The most common sonographic appearance of ILC is a hypoechoic mass with posterior acoustic shadowing. Other sonographic presentations include acoustic shadowing without any obvious mass, ill-defined area of altered, hypoechoic, inhomogeneous echotexture without identifiable margins, and frank shadowing. Less commonly ILC may present as single or multiple well-circumscribed masses. On ultrasound two classic signs of ILC were described. First, the Golden Gate sign is due to the involvement of a few adjacent Cooper‘s ligaments by cancer so that the shadowing area (hypoechoic area) resembles the shape of a suspension bridge. The second one named the picket fence sign is observed when multiple adjacent Cooper‘s ligaments are involved in cancer and the shadowing area resembles a picket fence. Rarely ILC may present as a hyperechoic mass on ultrasound which may be assigned a wrong benign diagnosis. Hyperechoic masses should be evaluated by using the same suspicious sonographic characteristics that are used to assess hypoechoic breast masses and indistinct or ill-defined margins of hyperechoic mass should raise the suspicion and prompt for histopathological correlation. Ultrasound is an invaluable adjunctive tool in cases of focal or developing asymmetry and may help in characterizing benign or suspicious lesions. However; the absence of a sonographic correlate can not completely exclude malignancy as occasionally ILC may be sonographically occult. MR imaging is superior to mammography and US for the diagnosis of ILC and in the estimation of tumor size, extent, and detection of multifocality and multicentricity At MR imaging, the most common manifestation of ILC is a solitary mass with spiculated or ill-defined margins. Additional manifestations include a single dominant lesion surrounded by multiple small enhancing foci, multiple lesions, either connected by enhancing strands or separated by nonenhancing intervening tissue, architectural distortions, regional or segmental non mass-like enhancement and only enhancing septations without any dominant mass as in our case. MRI is an important tool in the preoperative management and staging in cases of invasive lobular carcinoma.
Reference
References -1. Solid breast nodules: use of sonography to distinguish between benign and malignant lesions. A T Stavros, D Thickman, C L Rapp, M A Dennis, S H Parker, and G A Sisney Radiology 1995 196:1, 123-134. 2. Pure Lobular Carcinoma of the Breast Presenting as a Hyperechoic Mass: Incidence and Imaging Characteristics. Katie N. Jones, Maureen Magut, Tara L. Henrichsen, Judy C. Boughey, Carol Reynolds, and Katrina N. Glazebrook. American Journal of Roentgenology 2013 201:5, W765-W769. 3. Johnson K, Sarma D, Hwang ES. Lobular breast cancer series: imaging. Breast Cancer Res. 2015 Jul 11;17(1):94. doi: 10.1186/s13058-015-0605-0. PMID: 26163296; PMCID: PMC4499185. 4.Cawson, J.N., Law, E.-M. and Kavanagh, A.M. (2001), Invasive lobular carcinoma: Sonographic features of cancers detected in a BreastScreen Program. Australasian Radiology, 45: 25-30. https://doi.org/10.1046/j.1440-1673.2001.00867.x