




Findings
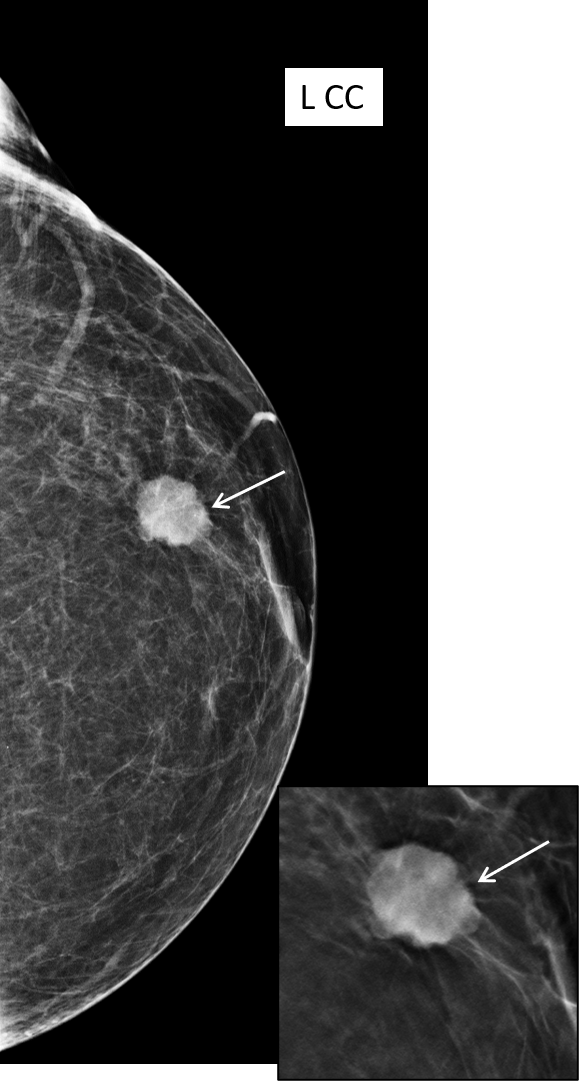
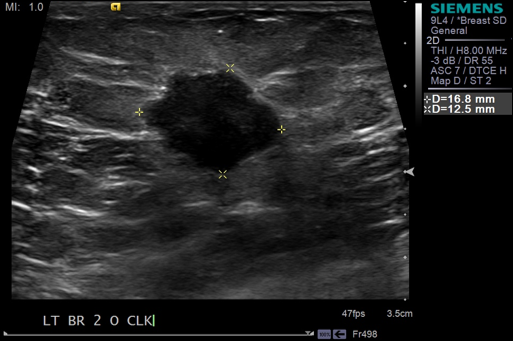
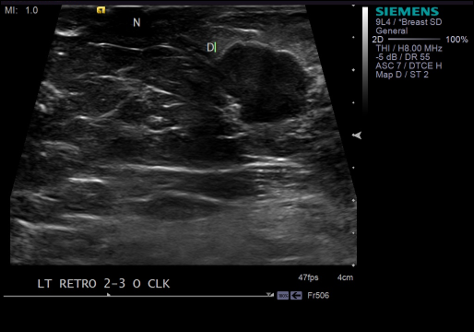
Which of the following characteristics describes the mass in the breast? a) High density mass with spiculated margins b) Isodense mass with lobulated margins c) Irregular isodense mass with indistinct margins posteriorly d) Circumscribed oval mass The appropriate choice is ‘c’ with the presence of an axillary lymph node. What would be your next step? a) Assign a BIRADS category and proceed to Biopsy b) MRI c) USG The next step would be ‘c’, to perform an ultrasound to further characterize the mass and determine vascularity. Which of the following characterizes the ultrasound features of the mass a) Solid mass with spiculated margins b) Irregular iso to hypoechoic mass with moderate posterior acoustic enhancement and internal vascularity c) Circumscribed iso to hypoechoic mass with moderate posterior acoustic enhancement The appropriate choice would be ‘b’. Which of the following characterizes the lymph node? a) Cortical thickening suggestive of benign process b) Cortical thickening suggestive of metastatic lymph node As the cortical thickening was 3.7 mm, a possibility for metastasis is likely.
Answer
What would be the final BIRADS category – BIRADS IV C A US-guided core needle biopsy was performed. Histology was consistent with papillary carcinoma breast. FNAC from axillary lymph node – Cytological features are suggestive of papillary carcinoma breast metastasis. Differential Diagnosis Fibroadenoma - circumscribed oval isodense mass, hypo to isoechoic on USG. Phyllodes tumor - dense mass on mammography. - circumscribed hypoechoic mass with cystic foci on USG. Invasive ductal carcinoma - IDC - IDC – NOS - Invasive special subtypes (medullary, mucinous) Spectrum of papillary neoplasm - Benign, papilloma with atypical features, carcinoma in situ, sclerosing papilloma.
Discussion
The above case is not the typical presentation of a papillary carcinoma as the patient is a young premenopausal woman, who presented with a breast lump not in the characteristic retroareolar location. The ultrasound also shows the less common irregular iso to hypoechoic mass with moderate posterior acoustic enhancement and internal vascularity. Axillary lymph nodal metastasis is also not commonly seen. As there is varied appearance of papillary carcinomas, they should be considered as a differential in relatively benign appearing tumors in the younger age group as well. Papillary carcinomas are rare tumors of the breast and comprise less than 2% of all breast carcinomas. They are more frequently seen in older post menopausal women. They are comparatively slow growing tumors with a better prognosis and 10 year survival rate of >95% Patients may present with a lump or more commonly with bloody or serosanguinous nipple discharge. The masses are commonly detected in the retroareolar region in about 50% of the patients. Axillary lymph nodal involvement is uncommon though enlarged nodes with sinus histiocytosis are encountered. Mastectomy with axillary node dissection is the treatment of choice with no adjuvant therapy. Papillary carcinomas are divided into solid, intracystic without invasion, intracystic with a focus of invasion (usually ductal carcinoma) and invasive papillary carcinoma. The absence of a myoepithelial layer differentiates carcinomas from benign papillary lesions. On Mammogram, they are usually circumscribed or partially circumscribed, round, oval or lobulated masses. The margins are most commonly well-defined. Indistinct margins are seen in areas of invasion. As there is no surrounding fibrotic reaction or minimal fibrotic reaction, spiculated margins are not typically seen in these masses. Microcalcifications within the tumor are commonly pleomorphic though coarse or heterogeneous calcifications may also be present. On USG, papillary carcinomas have a variable appearance and present as hypoechoic solid masses with moderate posterior acoustic enhancement, complex solid cystic mass with septations, complex cystic mass with papillary projections. Doppler demonstrates feeding vessels and intratumoral blood flow. On MRI, papillary carcinoma may appear as irregular enhancing lesions with enhancing nodules or complex cysts with enhancement. The MRI morphological features and kinetic curves of papillary carcinoma are not characteristic and may coincide with those of the benign lesions. MRI is a useful tool in evaluating the extent of disease, more so in the presence of multiple lesions. Core Biopsy versus surgical excision There is upgradation of benign papillary lesions diagnosed by core needle biopsy to malignancy in as much as 38% of the cases at the time of surgical excision. Therefore, in a scenario of clinically, radiologically or histologically worrisome features, surgical excision should be considered. Both benign and malignant lesions mimic papillary carcinomas. The appearance of papillary carcinoma varies in location and morphology on different imaging modalities, therefore tissue diagnosis with biopsy and radiological-pathological correlation is important to reach the correct diagnosis.
Reference
1. Diagnostic Breast Imaging – 2nd Edition, Berg. Yang 2. Papillary Lesions of the Breast: MRI, Ultrasound, and Mammographic Appearances – Riham Eiada, Jennifer Chong, Supriya Kulkarni, Frank Goldberg, Derek Muradali – AJR 2012; 198:264-271 3. Papillary carcinoma of the breast: Imaging findings – M S Soo, M E Williford, R Walsh, R C Bentley and P J Kornguth – AJR, Vol.164; Issue.2; Pages 321-326; Issue publication, date: Feb 1995 4. Papillary Carcinoma of the Breast: An Overview – Sumanta Kumar Pal, M.D., Sean K. Lau, M.D.,[…], and George Somlo, M.D., F.A.C.P. 5. Papillary lesions of the breast: A Review – Mulligan AM, O’Malley FP – Adv Anat Pathol , 2007; 14:108-119