


Findings
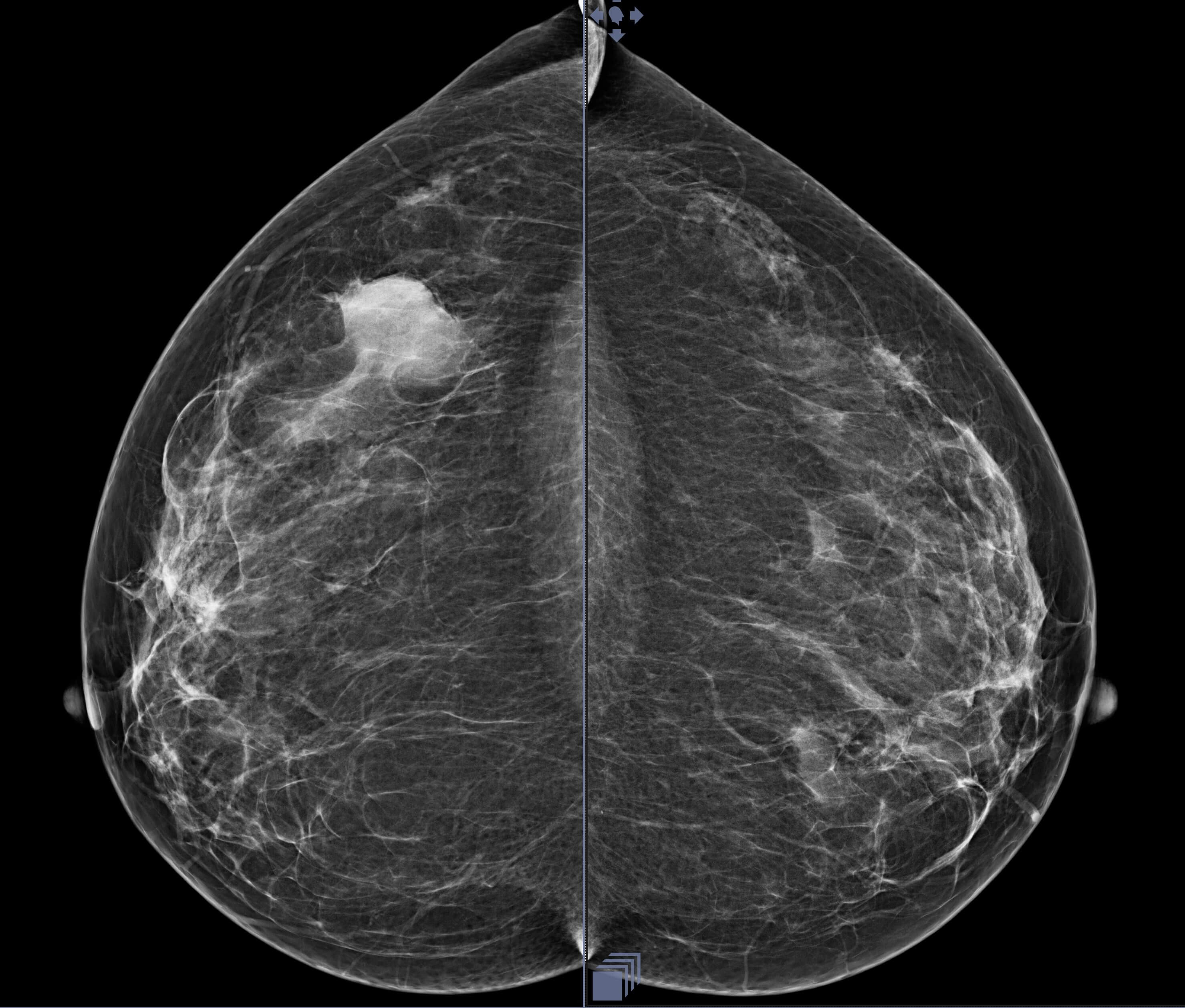
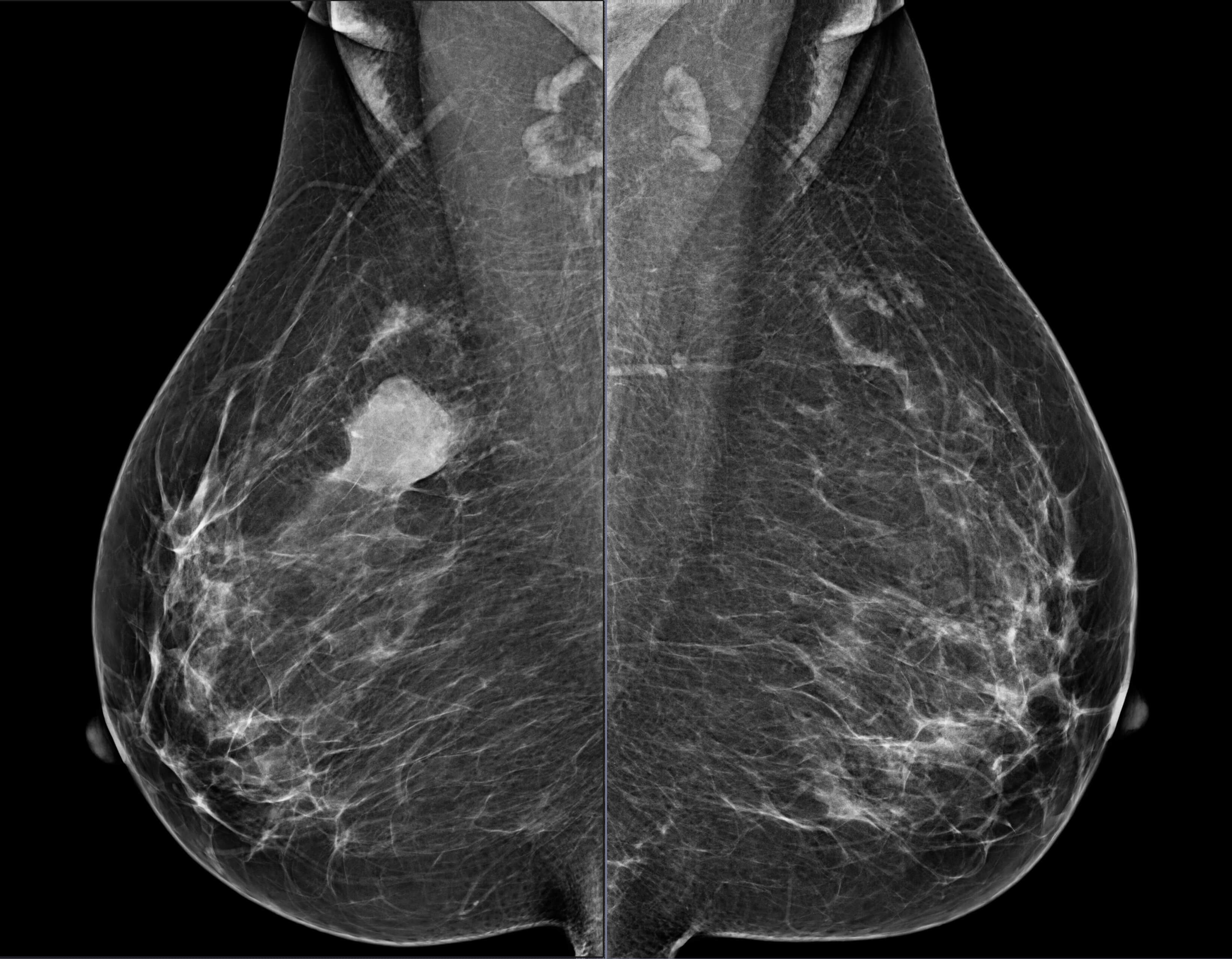
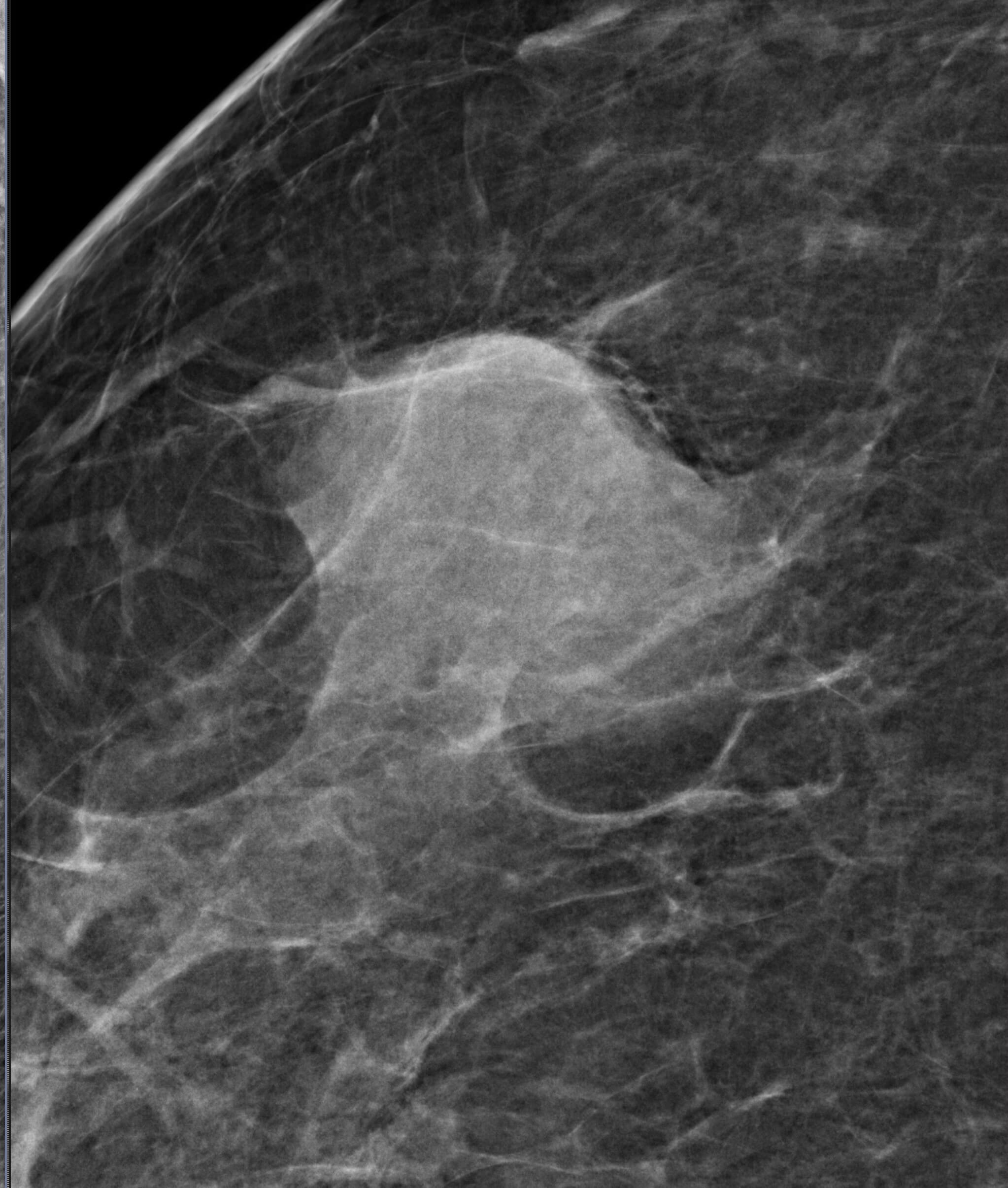
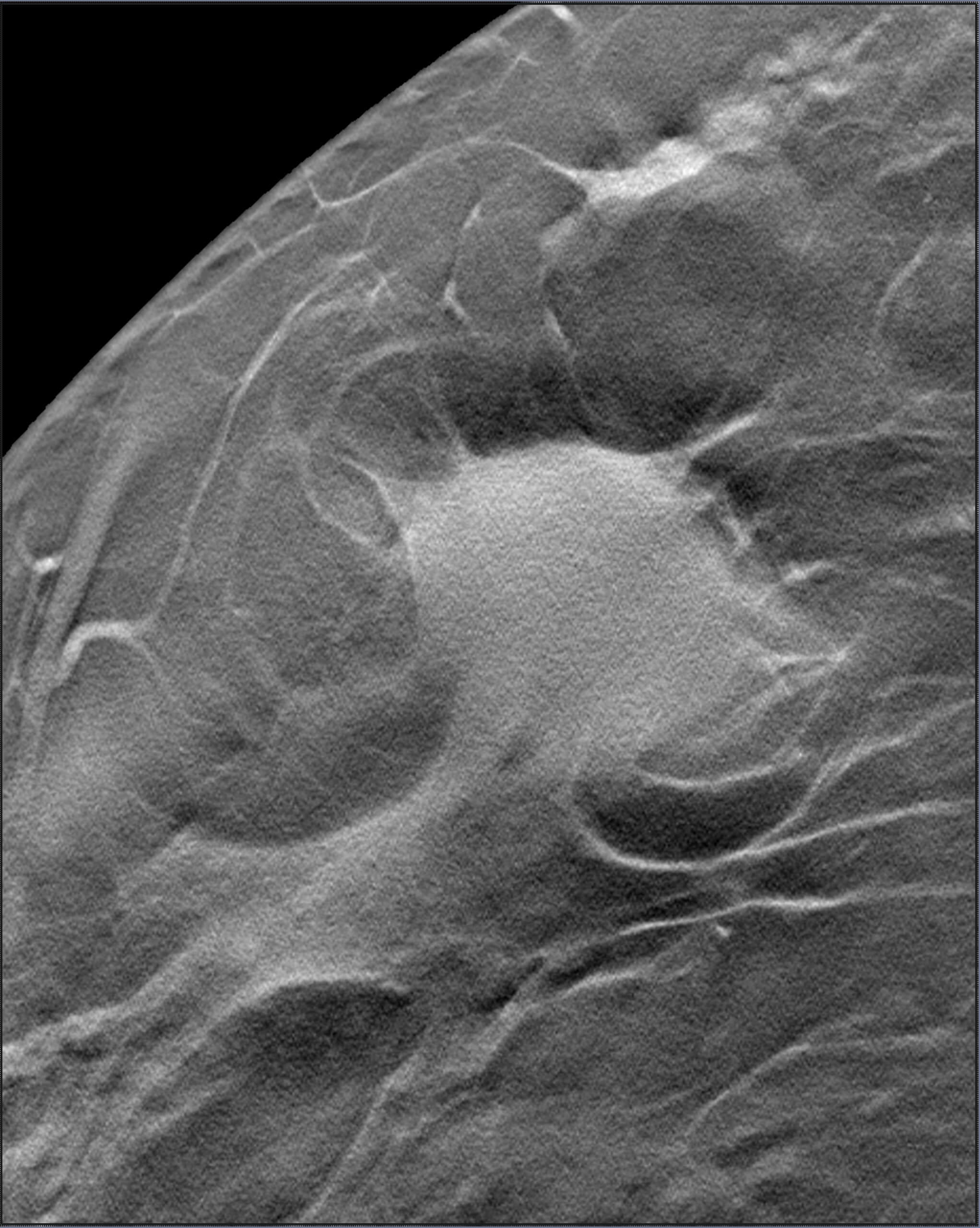
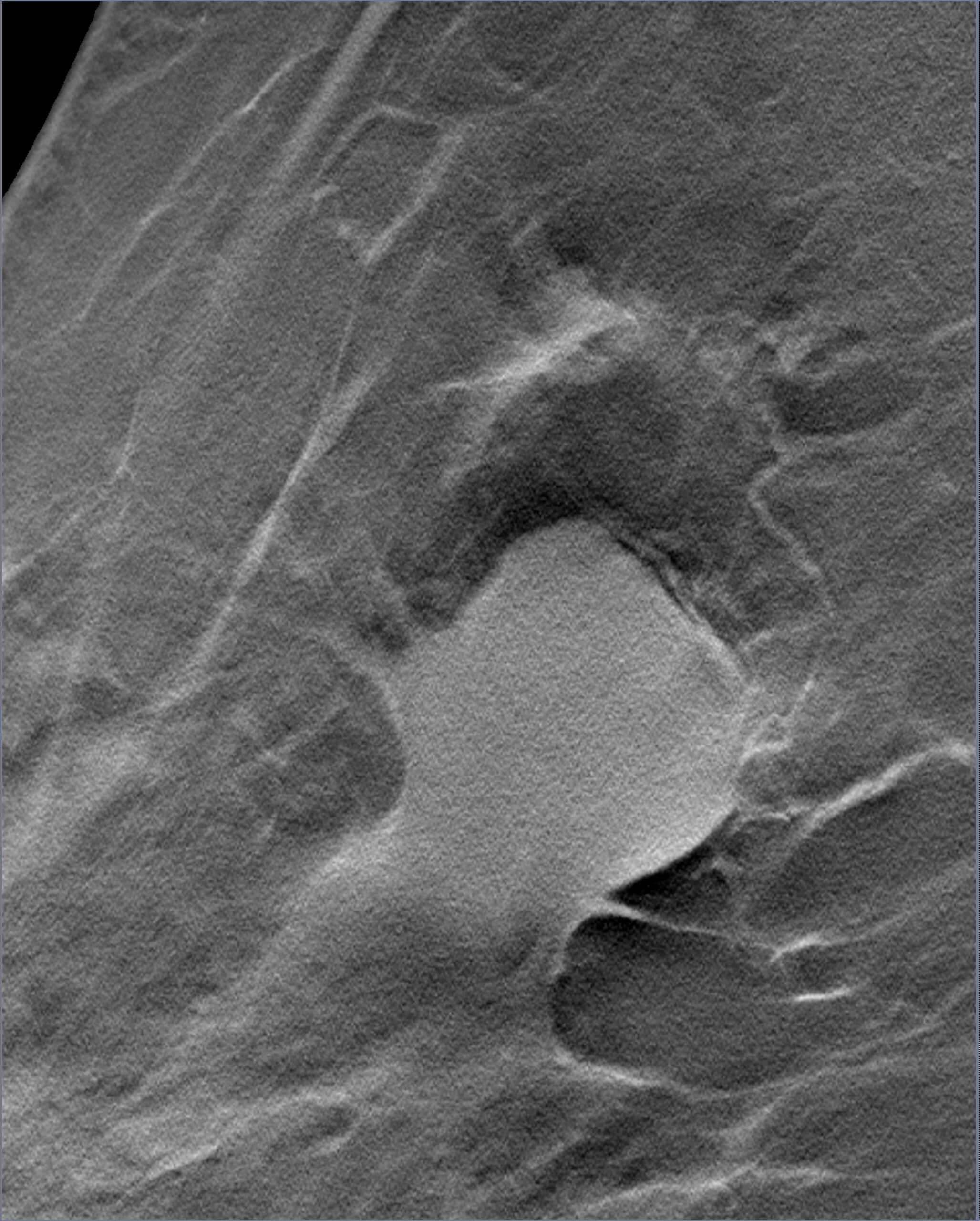
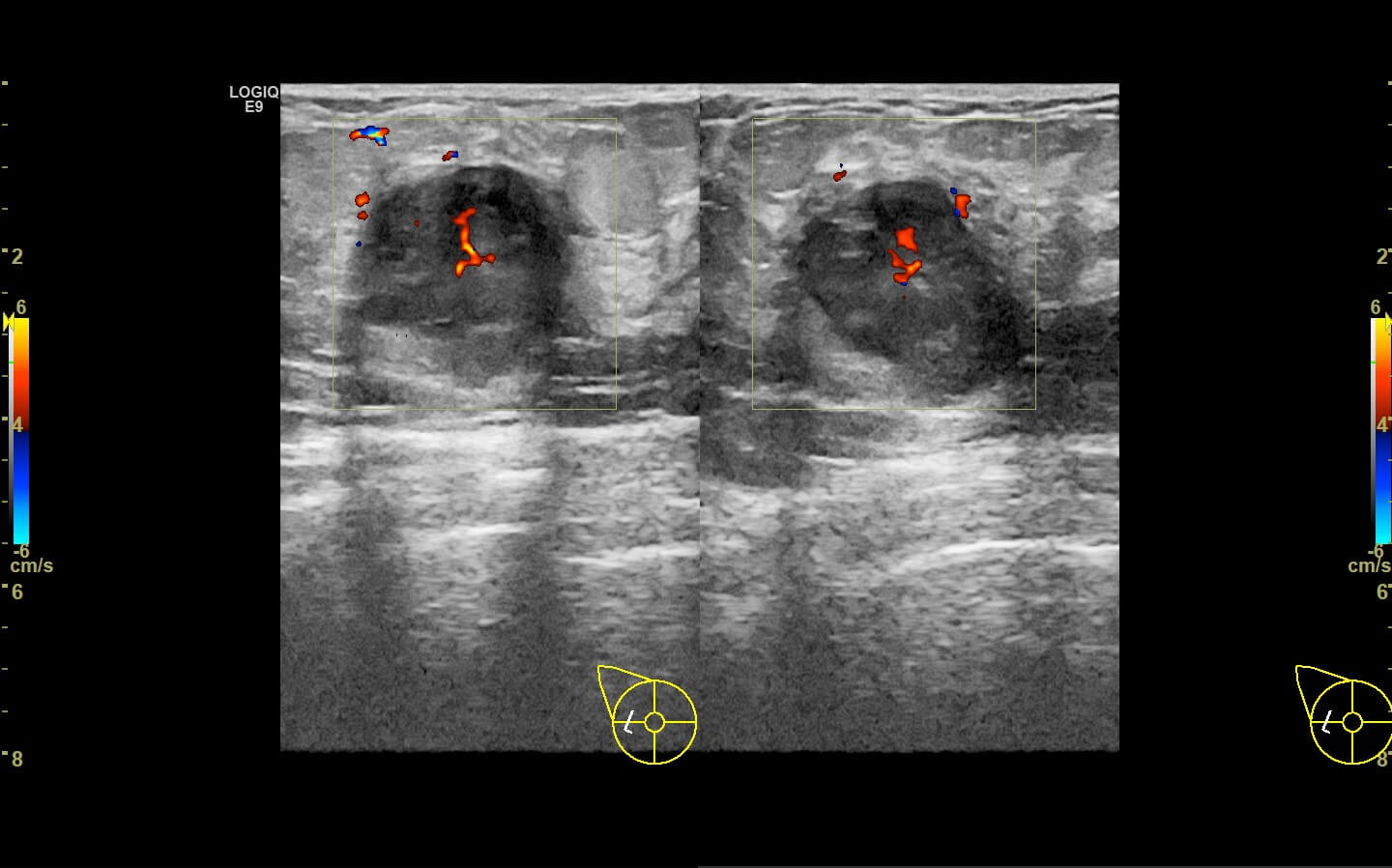
Mammogram revealed the presence of an irregular high density mass in the posterior third of the upper outer quadrant of the right breast with indistinct margins on two-dimensional mammogram. No internal calcification seen. No overlying skin thickening or retraction noted. DBT (Digital breast tomosynthesis) revealed the mass having spiculated margins and irregular shape. Corroborative ultrasound showed an irregular, heteroechoic solid mass at 10-11 O’clock position with anti-parallel orientation, microlobulated margins, posterior enhancement and internal necrotic/ cystic areas within. Mild internal vascularity was seen on color Doppler. No dilated ducts or intraductal extension was seen. No suspicious lymph nodes were present Further recommendation: Ultrasound guided core-needle biopsy with immunohistochemical analysis Management received: Right side lumpectomy with MRM Final histopathology: Metaplastic carcinoma (carcinosarcoma) with no nodal metastasis
Answer
Overall BI-RADS category 4B Differential diagnosis: Atypical or malignant phylloides, tumors like mucinous carcinoma, triple negative breast cancer, metaplastic carcinoma
Discussion
Metaplastic carcinoma (MPC) of breast is a heterogeneous group of neoplasm with mixed epithelial and mesenchymal differentiation. It is rare tumor, accounting for less than 5% of breast carcinomas and is associated with poor overall survival. The immunohistochemical analysis shows expression for markers of mesenchymal cells, epithelial cells and myoepithelial cells indicating MPC. The latter are not associated with estrogen/ progesterone/ HER2 neu markers. WHO classifies MPCs into epithelial and mixed type whereas Wargotz and Norris classified into five types based on the histopathology: i) Spindle cell type, ii) Squamous cell, iii) Carcinosarcoma, iv) Matrix producing, and v) MPC with osteoclastic giant cells. MPCs usually occur in females above 50 years of age as rapidly progressing tumors. These carry a high risk of haematogenous spread of malignancy than lymphatic spread and the predictors for poorer outcome include skin invasion, younger age at presentation (less than 39 years), appearance of squamous cells in the axillary lymph nodes. On imaging; the characteristic imaging features of more commonly seen Invasive ductal carcinoma(IDC) like irregular shape, spiculated margins, segmentally distributed pleomorphic calcifications are infrequent in MPCs. In addition, features like posterior acoustic shadowing and angular margins on ultrasound are also less commonly seen in the MPCs as compared to IDCs. Hence, they can resemble and misinterpreted as benign masses on imaging and thus high index of suspicion is required with clinic-radiological correlation while interpreting benign looking masses. This case highlights the varied imaging features of atypical breast malignancies and emphasizes the need for clinical correlation, image guided tissue sampling from solid-cystic masses and rad-path correlation for appropriate management of the patient.
Reference
1. Leddy R, Irshad A, Rumboldt T, Cluver A, Campbell A, Ackerman S. Review of metaplastic carcinoma of the breast: imaging findings and pathologic features. J Clin Imaging Sci. 2012;2:21. doi: 10.4103/2156-7514.95435. 2. Yang WT, Hennessy B, Broglio K, Mills C, Sneige N, Davis WG, Valero V, Hunt KK, Gilcrease MZ. Imaging differences in metaplastic and invasive ductal carcinomas of the breast. AJR Am J Roentgenol. 2007 Dec;189(6):1288-93. doi: 10.2214/AJR.07.2056. 3. Doshi DJ, March DE, Crisi GM, Coughlin BF. Complex cystic breast masses: diagnostic approach and imaging-pathologic correlation. Radiographics. 2007 Oct;27 Suppl 1:S53-64. doi: 10.1148/rg.27si075508. PMID: 18180235.